
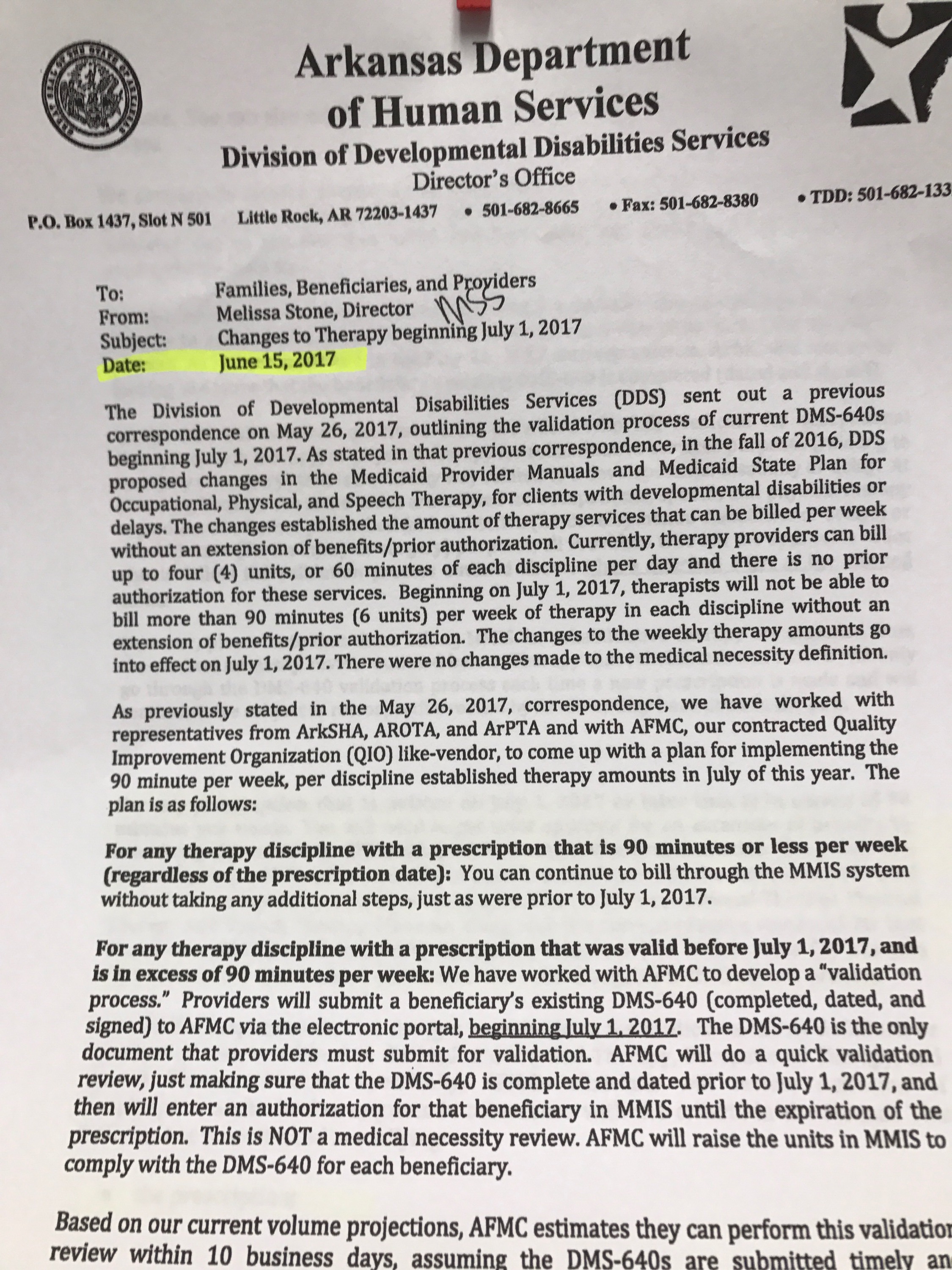
FYI – This letter was sent by Arkansas Department of Human Services DDS Division to all Waiver Providers today:


FYI – This letter was sent by Arkansas Department of Human Services DDS Division to all Waiver Providers today:
The PT, OT, and SH Association Presidents regularly meet with DHS and AFMC to discuss issues that providers have when requesting Prior Authorizations (PAs) for children who need therapy over the 90-minute cap. These are the results of their latest meeting.
Keep track of your questions and email them to be discussed at the next meeting.
The following are issues raised by members of ArkSHA, ArPTA and AROTA, and responses from AFMC and DDS.
Issue: Shifting of Units Between Therapist and Assistant
There are still questions regarding the length of time it is taking to shift units from PT/OT/ST to PTA/COTA/SLPA and vice versa. AFMC reports that following completion of the large number of DMS-640 form validations AFMC received many change requests to prior authorizations. AFMC encouraged their staff to continue to process initial DMS-640 validations and that all changes would need to be checked before processing. Currently, AFMC states that they are about 10 days out on corrections and Jarrod McClain, AFMC Director for Clinical Review, indicated that their staff are working diligently to get the updates made as quickly as possible. The updates to the PA’s flow to DXC each night and providers can start billing immediately upon receipt of the changes.
In addition, Jarrod stated that AFMC is working to decrease the timeframe for corrections but they have to ensure that they are getting the correct request ID modified. According to Jarrod, it takes a few days to check and update the claims data extract file. If providers continue to see a delay, please contact Jarrod McClain at AFMC. He will personally see that his staff checks on the status of their request and get it processed.
Issue: Use of evaluations from preschool programs to kindergarten
There was concern from many members as to how long their evaluations will be valid in a schools setting. The consensus is that if the evaluation utilized is an evaluation conducted by a non-educational agency, or by a provider who is not contracted by an educational agency, then the evaluation is good for one year. If an educational agency or a contractor of the educational agency conducted the evaluation, then the evaluation falls under the school-based evaluation criteria of every 3 years.
Issue: Some prior authorizations were only approved after sending in a cover sheet restating information included in the evaluation.
AFMC was aware of this issue and is working to improve their processes for approval. In the meantime, providers are encouraged to highlight justification for medical necessity in the evaluative reports, including statements about how the services recommended are under accepted standards of practice to treat the patient’s condition, how services are complex and will require the skilled services of a qualified therapist, and a statement about therapy prognosis (See Medicaid Manual Section II). Though a cover letter outlining these justifications is not required, providers are encouraged to consider using a cover letter attached to the evaluation to make these medical necessity statements more salient for reviewers.
Issue: Are reviewers actually reading the evaluations or just looking for technical language?
AFMC assured us that they are reading all evaluations. They perform both technical and administrative reviews in order to ensure that all requirements of the evaluative reports are included, as well as a medical necessity review to ensure that justification for medically based services is included.
Issue: I heard that AFMC was using nurse reviewers and not experienced pediatric therapists in each discipline. Is this true?
AFMC utilizes registered nurses to perform the initial reviews of all PA requests. If a request is denied than the request is assessed by an experienced licensed therapists specific to the discipline. If the therapist agrees with the denial it is then sent to a board certified pediatric physician for final review. If a provider does not agree with the denial or would like to request reconsideration they may do so by resubmitting the request.
Issue: What about beneficiaries who receive services from multiple providers for the same service?
AFMC and DDS continue to emphasize the need for care coordination for beneficiaries with multiple providers of the same modality (physical, occupational or speech therapy). Dr. Chad Rodgers, AFMC Medical Director, attended our meeting and reported that the pediatricians and PCPs he has been in contact with are interested in understanding what situations justify the appropriate signing off on multiple prescriptions. He asserts that although he can’t speak for all physicians he personally looks at every request for therapy services before signing them. He recognized that it is difficult to for most physicians to understand why a child needs multiple services. He and assistant director of DDS Elizabeth Pittman stated that it would be beneficial to state on the DMS-640 the specific need for a particular service and that the beneficiary will need the services of multiple therapists. AFMC and DDS are considering a change to the DMS-640 forms in the future to accommodate the different services provided within one discipline. Elizabeth Pittman reported that the new MMIS system (which has an anticipated implementation of summer of 2018) will be less burdensome on providers and will have the ability to disclose is the beneficiary is receiving services from other providers. Until then, providers need to ask during the intake process if the recipient is receiving therapy services from any other provider, and then coordinate as needed. According to Jarrod McClain, only 10 providers have bumped into challenges with the multiple provider issues thus far.
Issue: For short term scripts (i.e. ortho docs who write for 2-6 weeks) that then need an extension once the patient has had a follow-up recheck. What is the most efficient way to keep PA’s from having to be unnecessarily done?
Providers can simply go into Review Point, and click the extend button. The codes will be transferred over and the new prescription can be uploaded. Information about the progress of the patient and continued medical necessity should be included with the extension.
Issue: It has come to the attention of AFMC and DDS that some facilities are sending notices to parents that they should not allow services for their child in the school due to the need for a PA if the school and independent facility are both treating the beneficiary.
Although Medicaid is a “medical” assistance program, it recognizes the importance of school-based services. The federal Medicaid program actually encourages states to use funds from their Medicaid program to help pay for certain healthcare services that are delivered in the schools, providing that federal regulations are followed. The associations stand with AFMC and DDS that sending notices to parents regarding billing for services between schools and independent clinics is not recommended. IDEA laws require schools to provide services to beneficiaries if needed for educational purposes. Schools also must provide therapy that is medically necessary. Therapy services outside of the school setting should not replicate services provided by therapists contracted or working with the school.
Issue: A representative at DHS has stated that physical therapy re-eval codes are no longer a valid code as of July 1st. Has anything changed in the recent rule change?
Reevaluation codes are not currently and haven’t been a reimbursable code. The two billable codes for physical therapy services are 97001 and 97110.

In February 2017, DHS notified 500 people that they would be receiving the funding to come off of the waiver waiting list this year. They sent paperwork for each recipient to fill out. In July, they sent another letter.
As of today, barely 250 people have responded, and the rest are in danger of losing their chance to come off the waiting list.
Our state DHS had to request the additional 500 slots from a federal agency, and that agency, Centers for Medicare and Medicaid, finally granted it on August 22, 2017. In the meantime, DHS sent another letter this summer in order to reach the rest of the people who have not yet responded. They also began working on plans of care for those who have responded. Once a person responds, it will take 60-90 days to set up the Independent Assessment, the staff required for the plan of care, supplies, and possible residencies.
If you have already been communicating about your plan of care, you will most likely see some progress in September to October. It is important to note that the federal approval was holding up progress. If you had chosen the company who you’d like to work with, please know that they were only notified as soon as the federal approval came through. You should be hearing from them soon.
Those of you in the 500 who were notified in February should receive DHS’ final letter in the coming days. If you have not yet responded to DHS about your spot in the top 500, they will also attempt to reach you by phone. If they can’t reach you by phone, they will remove you from the list of 500 and move on to the next people waiting.
If you have questions about this, you can’t simply call any office. You must call these specific people:
– For the status of applications:
Merinesa Morris
(501) 683-0571
– For all other questions:
Regina Davenport
(501) 683-0575
If you are a person on the waiting list, a caregiver, or a provider of someone on the list, please share this to ensure that this information gets to the correct people.
Here is a copy of the letter that will be going out:


A new developmental screener will now be REQUIRED to determine if a child is eligible to go to rehabilitation centers like Easter Seals, Access, the Allen School, Peds Plus, etc.
Public comment ends tonight on this rule change – August 12, 2017! Take this chance to comment on rules that affect you! Read the manuals for things that might affect you, and then send your comments and questions to Shelby.Maldonado@dhs.arkansas.gov. Make sure to tell her which documents below you’re commenting on. If you need any help, just watch a video tutorial below.

Here are the important Screener Rule changes that you might want to read:
| DDS Standards for Certification, Investigation and Monitoring – Redline | DDS-Stnds-Redline.doc | DDS STANDARDS for Certification, Investigation, an Monitoring for Center-Based Community Services | 1. Summary DDTCS-CHMS 2. Info |
| CHMS-2-17 Provider Manual Update | CHMS-2-17up.doc | CHMS Manual mark up with changes. | 1. Summary DDTCS-CHMS 2. Info |
| DDTCS-2-17 Provider Manual Update | DDTCS-2-17up.doc | DDTCS Manual mark up with changes. | 1. Summary DDTCS-CHMS 2. Info |
EXAMPLE OF COMMENTS SENT:
My public comment on the new screen:
DDS-Stnds-Redline.doc – Section 502.R, 504.A
CHMS-2-17up.doc – Section 203.100 C2, 217, 218.300, 241.000 B6, 242.000 A,
DDTCS-2-17up.doc – 202.000 B
I am concerned about the lack of details, such as what type of screen this will be. How can a short screen determine whether my child’s functionality would benefit from day habilitation? Also, I ask for the credentials of the people performing the screen to be qualified clinicians.
I’m concerned that parents and physicians need training to ensure that disruption in services does not occur.
My public comment on the Opt in/Opt Out:
CHMS-2-17up.doc – Section 206,
DDTCS-2-17up.doc – 203.000, 204.000, 214.131A, 214.132, 215.100D,
I am concerned that in Opting out, a parent must relinquish the child’s IDEA rights for as long as the child attends that center and/or as long as that center chooses to be opted out. Ok top of that, I’m concerned that services could be disrupted, especially if a parent chooses not to relinquish those rights and must find another place of service. Also, this may remove the freedom of choice for the parent if there is not another place of service nearby. Last, I’m concerned that disruption of services might occur as a child is transitioned into the school system.
I’m concerned that parents, therapists, educators, and advocates need training to ensure that disruption in services does not occur.
Use this form below, and it will go to the correct DHS representative.
Public comment ends tonight – August 12, 2017! Take this chance to comment on rules that affect you! Read the manuals for things that might affect you, and then send your comments and questions to Shelby.Maldonado@dhs.arkansas.gov. Make sure to tell her which documents below you’re commenting on. If you need any help, just watch a video tutorial by clicking the red button below.

Here are the important BH Rule changes that you might want to read:
| INPPSYCH-1-17 Provider Manual Update | INPPSYCH-1-17up.doc | Manual Update for Inpatient Psychiatric Services for Under Age 21 |
| OBHS-1-17 Provider Manual Update | OBHS-1-17up.doc | Manual Update for Outpatient Behavioral Health Services |
| Residential Community Integration Program Certification | ResCommReintCert.doc | Residential Community Integration Program Certification |
As you may know, Independent Assessments will be required for any Medicaid recipient in Tier 2 or 3 for Behavioral Health or Developmental Disability Services of DHS, as well as other Medicaid populations in Arkansas.
Public comment for these rules ends tonight, August 12, 2017! Read the manuals for things that might affect you, and then send your comments and questions to Shelby.Maldonado@dhs.arkansas.gov. Make sure to tell her which documents below you’re commenting on. If you need any help, just watch a video tutorial by clicking the red button below.

| AR Independent Assessment Manual | AR_IA_July_17.doc | New manual for Independent Assessment | 1. IA Public Notice 2. IA Manual Summary 3. IA fiscal Impact |
See all of the manuals for Independent Assessments.
Optum (the company that DHS has contracted to do these assessments) has released the following resource to help you understand the Independent Assessment process.
Click on the image below to learn more:

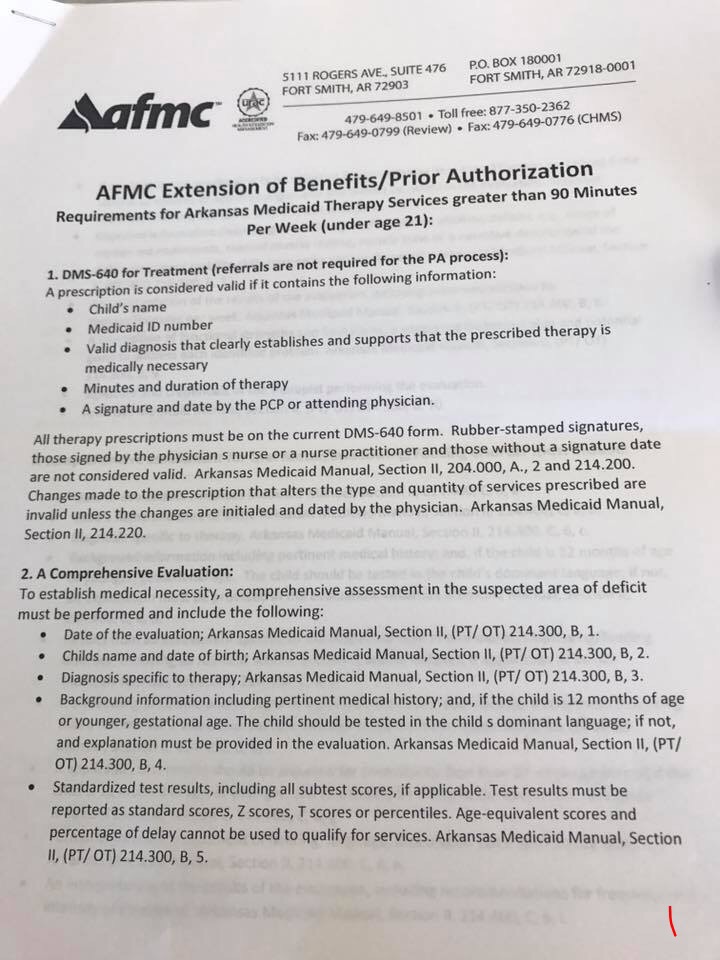
MSL has been made aware that there’s a lot of confusion on submitting PAs to request more than 90 minutes of therapy for children since the therapy cap was implemented on July 1, 2017. Lainey has talked with AFMC and DHS as well as the OT Association President who has been successful in submissions.
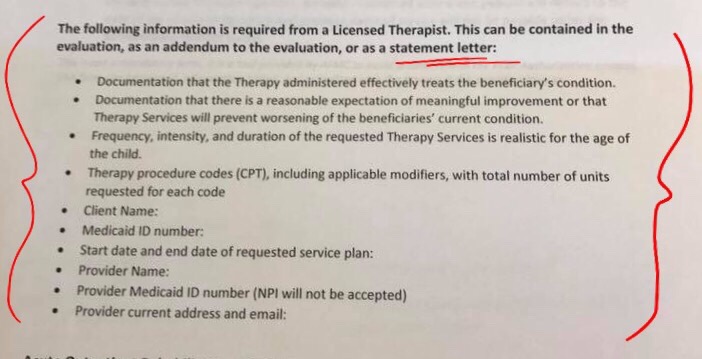
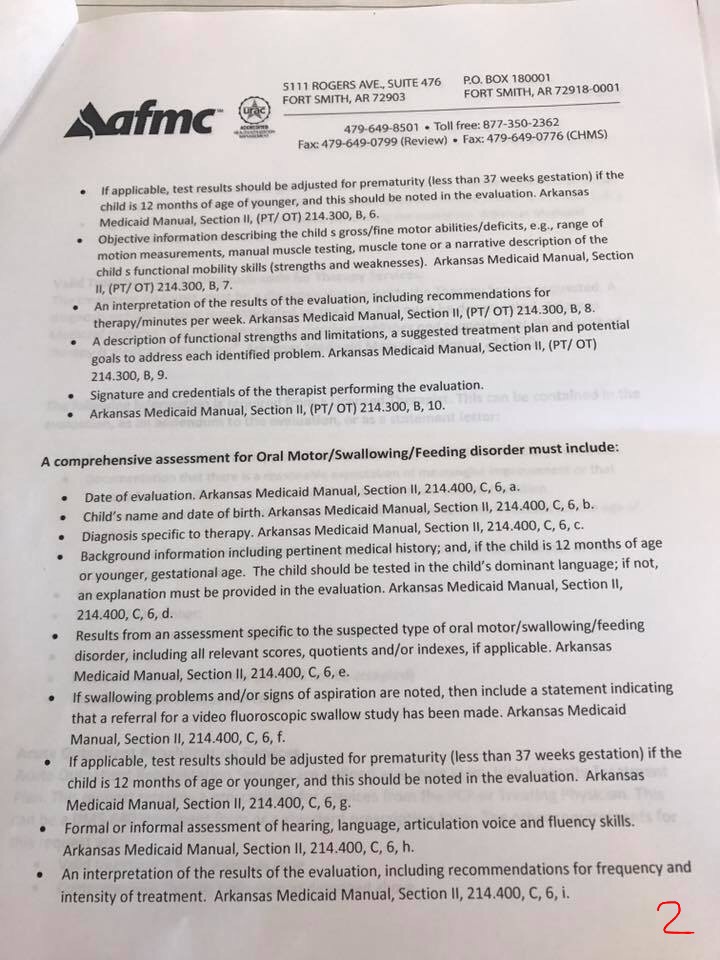
You need a separate statement letter that answers the following questions individual to the child’s case:
1. How does the therapy administered effectively treat the beneficiary’s condition?
2. What gives you a reasonable expectation that the beneficiary is experiencing meaningful improvement or that the therapy is preventing worsening of the beneficiary’s current condition?
3. How are the frequency, intensity, and duration of the requested therapy services realistic for the age of the child?
List the question and provide the answer. Make sure you provide the other information listed there as well. AFMC told Lainey today that they will deny any submission that does not have this requirement. If you have received denial with 3 statements that say you didn’t meet the requirement, try resubmitting with this.



DHS has released a manual/rule change for public comment until August 11, 2017. After that, you will not be able to get your comments on the record. In addition, they are hosting a public hearing on August 8.

You should read the manual for yourself to make sure you cover everything that concerns you. However, even if you read it, you might still wonder what to say. The comments below are an example of what one person plans to send in.
EXAMPLE | EXAMPLE | EXAMPLE | EXAMPLE | EXAMPLE | EXAMPLE | EXAMPLE
This is my public comment regarding PASSE-New-17up.doc:
Section 211.000 – It says that the PASSEs should begin October 1, 2017. I believe that this model is not ready to begin taking on clients for several reasons. Rules like this one still have to be sent through the legislature for their approval. The Insurance Department isn’t supposed to approve the PASSEs until mid-September, which will only leave them a couple of weeks before they start managing people’s care. We don’t know what the rules will be, and we don’t know who the PASSEs will be. If the PASSEs aren’t ready and don’t do a good job, they could make mistakes. This will hurt people. I want DHS to push the date back and allow us to keep things the way they are until the PASSEs have had adequate time to review all of the finalized rules and to hire and train people who understand the rules.
Section 214.000 – It says that people can choose another PASSE during the first 90 days and once every year. How will we know what the differences between each PASSE is? I want to pick the best PASSE, but I don’t understand all of the rules or what they all offer. (At this point, I have reason to wonder if the PASSEs themselves understand the rules, as they have not been finalized.) It also says “on the beneficiary’s annual anniversary of attribution to a PASSE.” Is this a single day to respond, or is it a week? You need to define how long that amount of time would be.
Section 214.000 D – It says a client can move because of “poor quality of care,” but how do we prove that? That is a relative term. Who determines what kind of care is poor? I believe that the patient should determine whether care is poor and what that means in their situation.
Section 215.000 – What if the abeyance is due to DHS/Medicaid’s fault in paperwork (and the client can prove that)? Will the coordinator help the recipient to know that their Medicaid eligibility is in dispute and help them to figure that out?
Section 222.000 G – “The right to be provided written notice of a change in the beneficiaries care coordination” should be at least 14 days, not 7 days. If you are relying on snail mail, half of the time can be used simply in sending the notification, leaving the receiver very little time to respond or make other arrangements. Why isn’t this policy the same as 223.000 B, allowing 30 days from the time it goes into effect?
Section 231.000 – The travel times and distances listed need to be cut in half, especially for DD and BH providers who are seen on a more frequent basis. For example, it is not in the best interest of a child or adult to have to travel an hour to and then an hour to return from a location to see a therapist multiple times per week.
Section 241 G, 242 A, & 243.000 – DHS needs to give the PASSEs enough money to have a qualified individual available to help me whenever I need them, as many times as I may need them. Many providers seem to be concerned that the amount announced at the AR Waiver Conference (in July 2017) of $177 is not enough. I want them to get what they need so they can give me what I need. After December 31, 2018, they should have a different funding source and should not use any money from recipients’ care for administrative funding needs.
Section 242.000 – It says in the document that care coordinators will be employees of the PASSE (241 B). However, it does not say where the care coordinators should be located. Because Arkansas is so rural, care coordinators located in the communities they serve would be most knowledgeable for their clients.
Section 254.000 – Will DHS be required to submit the data received from PASSEs, such as data that shows savings or lack thereof, for public viewing? We want to see that data as well.
Section 261.000 – This says that grievances must be resolved within 30 days of the filing date. What will happen in the meantime? If a person needs treatment, do they have to wait all that time to receive it?
Section 264.000 – This description needs more definition. Who may serve on a Consumer Advisory Council? I believe that beneficiaries or direct consumers should serve, but caregivers who speak in place of beneficiaries who can’t speak for themselves should also be able to serve.
 DHS released several manuals to the Medicaid website on July 13, 2017 that are available for public comment until August 11. Once public comment ends, these rules will be sent through the legislative committees and passed as law.
DHS released several manuals to the Medicaid website on July 13, 2017 that are available for public comment until August 11. Once public comment ends, these rules will be sent through the legislative committees and passed as law.
“In accordance with federal and state law, the Division of Medical Services of the Arkansas Department of Human Services must advertise and make available for public comment proposed new and amended rules and other documents, such as certain initial waiver requests and waiver renewals.”
However, they released over 60 documents actually, which may have left you feeling confused about which one needs your comment or what’s in them all. Here’s your guide to wading through the state terminology and legalese.
RULE #1: When you send in your comments, make sure to list the document that you wish to comment on!
RULE #2: Make sure you send your comments to the appropriate person.
Send your comments to Shelby.Maldonado@dhs.arkansas.gov, and as long as you’ve included the right document title, she will be able to direct it to the correct person.

Instead of scrolling through the long table, which can be confusing, this list of topics can get you straight to what you want to see. Click the link to go directly to the corresponding manual in the table.
The following table will attempt to explain what each document is (memo, explanation letter, mark up with changes, or new manual), what it contains, and possibly some documents to assist you. Remember, the list of topics above can assist you in finding what you need much faster.
| Document Title | Document | Description | Assisting docs/info |
| Interested Persons and Providers Letter for DDS Standards for Certification, Investigation and Monitoring; State Plan Amendment 2017-011; Child Health Management Services provider manual update; and Developmental Day Treatment Clinic Services provider manual update | IPLtrSPA17-011.doc | memo | |
| (SPA011 – 1 of 15) | |||
| State Plan Amendment 2017-011 Attachment 3.1A 1i | SPA17-011-31A1i.doc | STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT: AMOUNT, DURATION AND SCOPE OF SERVICES PROVIDED, CATEGORICALLY NEEDY (page as it will appear in new manual) |
|
| (SPA011 – 2 of 15) | Page 1i | ||
| State Plan Amendment 2017-011 Attachment 3.1A 1i with tracked changes | SPA17-011-31A1i-markup.doc | SAME MANUAL PAGE: mark up that shows changes | |
| (SPA011 – 3 of 15) | Page 1i | ||
| State Plan Amendment 2017-011 Attachment 3.1A 4A | SPA17-011-31A4A.doc | STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT: AMOUNT, DURATION AND SCOPE OF SERVICES PROVIDED, CATEGORICALLY NEEDY (page as it wil appear in new manual) |
|
| (SPA011 – 4 of 15) | Page 4a | ||
| State Plan Amendment 2017-011 Attachment 3.1A 4A with tracked changes | SPA17-011-31A4A-markup.doc | SAME MANUAL PAGE: mark up that shows changes | |
| (SPA011 – 5 of 15) | Page 4a | ||
| State Plan Amendment 2017-011 Attachment 3-1B 2h | SPA17-011-31B2h.doc | STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT: AMOUNT, DURATION AND SCOPE OF SERVICES PROVIDED, MEDICALLY NEEDY (page as it wil appear in new manual) |
|
| (SPA011 – 6 of 15) | Page 2h | ||
| State Plan Amendment 2017-011 Attachment 3-1B 2h | SPA17-011-31B2h-markup.doc | SAME MANUAL PAGE: mark up that shows changes | |
| (SPA011 – 7 of 15) | Page 2h | ||
| State Plan Amendment 2017-011 | SPA17-011-31B4b.doc | STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT: AMOUNT, DURATION AND SCOPE OF SERVICES PROVIDED, MEDICALLY NEEDY (page as it wil appear in new manual) |
|
| (SPA011 – 8 of 15) | Page 4b | ||
| State Plan Amendment 2017-011 | SPA17-011-31B4b-markup.doc | SAME MANUAL PAGE: mark up that shows changes | 1. IA Public Notice 2. IA Manual Summary 3. IA fiscal Impact |
| (SPA011 – 9 of 15) | Page 4b | ||
| DDS Standards for Certification, Investigation and Monitoring – Redline | DDS-Stnds-Redline.doc | DDS STANDARDS for Certification, Investigation, an Monitoring for Center-Based Community Services | 1. Summary DDTCS-CHMS 2. Info |
| (SPA011 – 10 of 15) | entire manual, mark up that shows changes | ||
| DDS Standards for Certification, Investigation and Monitoring | DDS-Stnds-Clean.doc | DDS STANDARDS for Certification, Investigation, an Monitoring for Center-Based Community Services | |
| (SPA011 – 11 of 15) | entire manual, as it will appear | ||
| CHMS-2-17 Provider Manual Update Transmittal Letter | CHMS-2-17.doc | letter that explains which parts of the CHMS manual have been changed | |
| (SPA011 – 12 of 15) | |||
| CHMS-2-17 Provider Manual Update | CHMS-2-17up.doc | CHMS Manual mark up with changes. | 1. Summary DDTCS-CHMS 2. Info |
| (SPA011 – 13 of 15) | |||
| DDTCS-2-17 Provider Manual Update Transmittal Letter | DDTCS-2-17.doc | letter that explains which parts of the DDTCS manual have been changed | |
| (SPA011 – 14 of 15) | |||
| DDTCS-2-17 Provider Manual Update | DDTCS-2-17up.doc | DDTCS Manual mark up with changes. | 1. Summary DDTCS-CHMS 2. Info |
| (SPA011 – 15 of 15) | |||
| Interested Persons and Providers Letter for State Plan Amendment 2017-010, Outpatient Behavioral Health Services and Inpatient Psychiatric Provider Manual Updates and Residential Community Reintegration Program Certification | IPLtrSPA17-010.doc | memo | |
| (SPA010 – 1 of 8) | |||
| State Plan Amendment 2017-010 Attachment 3.1 A | SPA010-Attach3-1A.doc | STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT: AMOUNT, DURATION AND SCOPE OF SERVICES PROVIDED, CATEGORICALLY NEEDY (page as it will appear in new manual – NO MARK UP AVAILABLE) |
|
| (SPA010 – 2 of 8) | Page 6c17a | ||
| State Plan Amendment 2017-010 Attachment 3.1 B | SPA010-Attach3-1B.doc | STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT: AMOUNT, DURATION AND SCOPE OF SERVICES PROVIDED, MEDICALLY NEEDY (page as it will appear in new manual – NO MARK UP AVAILABLE) |
|
| (SPA010 – 3 of 8) | Page 5f17a | ||
| Residential Community Integration Program Certification | ResCommReintCert.doc | Residential Community Integration Program Certification | |
| (SPA010 – 4 of 8) | entire manual as it will appear NO MARK UP AVAILABLE | ||
| Inpatient Psychiatric (INPPSYCH-1-17) Provider Manual Update Transmittal Letter | INPPSYCH-1-17.doc | Letter that shows the changes to Manual Update for Inpatient Psychiatric Services for Under Age 21 | |
| (SPA010 – 5 of 8) | |||
| INPPSYCH-1-17 Provider Manual Update | INPPSYCH-1-17up.doc | Manual Update for Inpatient Psychiatric Services for Under Age 21 | |
| (SPA010 – 6 of 8) | entire manual as it will appear NO MARK UP AVAILABLE | ||
| Outpatient Behavioral Health Services (OBHS-1-17) Provider Manual Update Transmittal Letter | OBHS-1-17.doc | Letter that shows the changes to Manual Update for Outpatient Behavioral Health Services | |
| (SPA010 – 7 of 8) | |||
| OBHS-1-17 Provider Manual Update | OBHS-1-17up.doc | Manual Update for Outpatient Behavioral Health Services | |
| (SPA010 – 8 of 8) | entire manual, mark up that shows changes | ||
| Interested Persons and Providers Letter for Independent Assessment Manual | IPLtrAR_IA.doc | memo | |
| (AR_IA – 1 of 2) | |||
| AR Independent Assessment Manual | AR_IA_July_17.doc | New manual for Independent Assessment | 1. IA Public Notice 2. IA Manual Summary 3. IA fiscal Impact |
| (AR_IA – 2 of 2) | |||
| Interested Persons and Providers Letter for DDS Policy 1076 -Appeals | IPLtrDDS1076.doc | memo | |
| (1076 – 1 of 3) | |||
| DDS Policy 1076 with Tracked Changes | DDS1076-Appeals-markup.doc | DDS Policy APPEALS Manual | |
| (1076 – 2 of 3) | entire manual, mark up that shows changes | 1. Summary Appeals 2. Info Policy 1076 Appeals |
|
| DDS Policy 1076 -Clean | DDS1076-Appeals-clean.doc | DDS Policy APPEALS Manual | |
| (1076 – 3 of 3) | entire manual, as it will appear | ||
| Interested Persons and Providers Letter for DDS Policy 1086 | IPLtrDDS1086.doc | memo | |
| (DDS1086 – 1 of 3) | |||
| DDS Policy 1086 with tracked changes | DDS1086-HDC-markup.doc | DDS Human Development Center Admission and Discharge Rules Policy Manual | |
| (DDS1086 – 2 of 3) | entire manual, mark up that shows changes | 1. 1086 HDC Rules Summary
2. 1086 Info |
|
| DDS Policy 1086 | DDS1086-HDC.doc | DDS Human Development Center Admission and Discharge Rules Policy Manual | |
| (DDS1086 – 3 of 3) | entire manual, as it will appear | ||
| Interested Persons and Providers Letter for Medical Services Policy Manual Sections E-600 through E-670 and Appendix R | IPLtrABLE.doc | memo | |
| (ABLE – 1 of 2) | |||
| Medical Services Policy Manual Sections E-600 through E-670 and Appendix R | ABLE.pdf | Able Act Policy Manual: Eligibility Factors, Contributions, Withdrawals, Expenses, Exclusions, | |
| (ABLE – 2 of 2) | entire manual, as it will appear – NO MARK UP AVAILABLE | ||
| Interested Persons and Providers Letter for Community and Employment (CES) 1915 (c) Waiver, DDSCES-1-17 Provider Manual Update and Certification Standards for CES Providers | IPLtrDDSCES.doc | memo | C Waiver |
| (CES – 1 of 5) | |||
| DDS Community and Employment Supports (CES) Waiver Minimum Certification Standards | DDSCESCertStand-markup.doc | DDS Community and Employment Supports (CES) Waiver Minimum Certification Standards | |
| (CES – 2 of 5) | entire manual, mark up that shows changes | 1. Summary of Changes | |
| DDS Community and Employment Supports (CES) Waiver Minimum Certification Standards | DDSCESCertStand.doc | DDS Community and Employment Supports (CES) Waiver Minimum Certification Standards | |
| (CES – 3 of 5) | entire manual, as it will appear | ||
| Developmental Disabilities Services Community and Employment Supports (DDSCES1-17) Provider Manual Update Transmittal Letter | DDSCES-1-17.doc | Letter that shows the changes to Manual Update for Arkansas Medicaid Health Care Providers – DDS Community and Employment Supports (CES) | |
| (CES – 4 of 5) | |||
| DDSCES-1-17 Provider Manual | DDSCES-1-17up.doc | Manual Update for Arkansas Medicaid Health Care Providers – DDS Community and Employment Supports (CES) | |
| (CES – 5 of 5) | entire manual, mark up that shows changes | 1. Summary of Changes 2. Info – CES Waiver |
|
| Interested Persons and Providers Letter for Provider-Led Arkansas Shared Savings Entity (PASSE) Waiver and New Provider Manual | IPLtrPASSE.doc | memo | |
| (PASSE 1 of 5) | |||
| Provider-led Arkansas Shared Savings Entity Program – Phase I | PASSEWvr.pdf | PASSE Program Information | B Waiver 1. Summary of PASSE 2. Info & Financial Impact |
| (PASSE 2 of 5) | |||
| Provider-led Arkansas Shared Savings Entity Spreadsheet | SpreadsheetPASSEWvr.pdf | PASSE Information – Enrollment Projections, Costs | |
| (PASSE 3 of 5) | |||
| PASSE-New-17 Provider Manual Update Transmittal Letter | PASSE-New-17.doc | letter that explains Provider-Led Arkansas Shared Savings Entity (PASSE) Program manual | |
| (PASSE 4 of 5) | |||
| PASSE-New-17 Provider Manual Update | PASSE-New-17up.doc | New PASSE Manual | |
| (PASSE 5 of 5) | entire manual, mark up | 1. Summary of PASSE 2. Info & Financial Impact |
|
| Interested Persons and Providers Letter for Independent Assessment for Personal Care and Criminal Background Check Requirements for Providers | IPLtrIA.doc | memo | |
| (IA – 1 of 22) | |||
| State Plan Amendment 2017-009 with Tracked Changes | SPA17-009-markup.doc | STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT: AMOUNT, DURATION AND SCOPE OF SERVICES PROVIDED, CATEGORICALLY NEEDY (mark up that shows changes |
|
| (IA – 2 of 22) | Page 10aa | ||
| State Plan Amendment 2017-009 | SPA17-009.doc | SAME MANUAL PAGE: as it will appear | |
| (IA – 2 of 22) | Page 10aa | ||
| ARChoices in Home Care Home and Community-Based 2176 Waiver (ARCHOICES-1-17) Provider Manual Update Transmittal Letter | ARCHOICES-1-17.doc | letter that explains changes to ARChoices In Homecare Home and Community-Based 2176 Waiver Manual | |
| (IA – 3 of 22) | |||
| ARCHOICES-1-17 Provider Manual Update | ARCHOICES-1-17up.doc | ARChoices In Homecare Home and Community-Based 2176 Waiver Manual | |
| (IA – 4 of 22) | entire manual, mark up that shows changes | ||
| Child Health Services/Early and Periodic Screening, Diagnosis, and Treatment (EPSDT-1-17) Provider Manual Update Transmittal Letter | EPSDT-1-17.doc | letter that explains changes to Arkansas Medicaid Health Care Providers – EPSDT Manual | |
| (IA – 5 of 22) | |||
| EPSDT-1-17 Provider Manual Update | EPSDT-1-17up.doc | Arkansas Medicaid Health Care Providers – EPSDT Manual change | |
| (IA – 6 of 22) | Section II, mark up that shows changes | IA required for certain home health clients 1. IA Public Notice 2. IA Manual Summary 3. IA fiscal Impact |
|
| Home Health (HOMEHLTH-1-17) Provider Manual Update Transmittal Letter | HOMEHLTH-1-17.doc | letter that explains changes to Arkansas Medicaid Health Care Providers – Home Health Manual | |
| (IA – 7 of 22) | |||
| HOMEHLTH-1-17 Provider Manual Update | HOMEHLTH-1-17up.doc | Arkansas Medicaid Health Care Providers – Home Health Manual change | |
| (IA – 8 of 22) | Section II, mark up that shows changes | background check changes | |
| Hospice (HOSPICE-1-17) Provider Manual Update Transmittal Letter | HOSPICE-1-17.doc | letter that explains changes to Arkansas Medicaid Health Care Providers – Hospice Service manual | |
| (IA – 9 of 22) | |||
| HOSPICE-1-17 Provider Manual Update | HOSPICE-1-17up.doc | Arkansas Medicaid Health Care Providers – Hospice Service manual changes | |
| (IA – 10 of 22) | Section II, mark up that shows changes | background check, IAs for personal care 1. IA Public Notice 2. IA Manual Summary 3. IA fiscal Impact |
|
| IndependentChoices (INCHOICE-1-17) Provider Manual Update Transmittal Letter | INCHOICE-1-17.doc | letter that expains changes to Arkansas Medicaid Health Care Providers – IndependentChoices Manual | |
| (IA – 11 of 22) | |||
| INCHOICE-1-17 Provider Manual Update | INCHOICE-1-17up.doc | Arkansas Medicaid Health Care Providers – IndependentChoices Manual changes | |
| (IA – 12 of 22) | Section II, mark up that shows changes | various changes included background checks | |
| Personal Care (PERSCARE-1-17) Provider Manual Update Transmittal Letter | PERSCARE-1-17.doc | letter that explains changes to Arkansas Medicaid Health Care Providers – Personal Care manual | |
| (IA – 13 of 22) | |||
| PERSCARE-1-17 Provider Manual Update | PERSCARE-1-17up.doc | Arkansas Medicaid Health Care Providers – Personal Care Manual changes | |
| (IA – 14 of 22) | Section II, mark up that shows changes | ||
| Private Duty Nursing Services (PDN-1-17) Provider Manual Update Transmittal Letter | PDN-1-17.doc | letter that explains changes to the Arkansas Medicaid Health Care Providers – Private Duty Nursing Services manual | |
| (IA – 15 of 22) | |||
| PDN-1-17 Provider Manual Update | PDN-1-17up.doc | Arkansas Medicaid Health Care Providers – Private Duty Nursing Services Manual changes | |
| (IA – 15 of 22) | Section II, mark up that shows changes | background checks | |
| Physician (PHYSICN-3-17) Provider Manual Update Transmittal Letter | PHYSICN-3-17.doc | letter that explains changes to the Physician/ Independent Lab/CRNA/Radiation Therapy Center manual | |
| (IA – 17 of 22) | |||
| PHYSICN-3-17 Provider Manual Update | PHYSICN-3-17up.doc | Physician/ Independent Lab/CRNA/Radiation Therapy Center manual changes | |
| (IA – 18 of 22) | Section II, mark up that shows changes | IA requirement 1. IA Public Notice 2. IA Manual Summary 3. IA fiscal Impact |
|
| Rural Health Clinic (RURLHLTH-1-17) Provider Manual Update Transmittal Letter | RURLHLTH-1-17.doc | letter that explains changes to the Rural Health Clinic Services manual | |
| (IA – 19 of 22) | |||
| RURLHLTH-1-17 Provider Manual Update | RURLHLTH-1-17up.doc | Rural Health Clinic Services manual changes | |
| (IA – 20 of 22) | Section II, mark up that shows changes | IA requirement 1. IA Public Notice 2. IA Manual Summary 3. IA fiscal Impact |
|
| Section I (SecI-3-17) All Provider Manuals Update Transmittal Letter | SecI-3-17.doc | letter that explains the changes to the Arkansas Medicaid Health Care Providers – All Providers manual | |
| (IA – 21 of 22) | |||
| SecI-3-17 All Provider Manuals Update | SecI-3-17up.doc | Arkansas Medicaid Health Care Providers – All Providers manual | |
| (IA – 22 of 22) | Section II, mark up that shows changes | IA requirement 1. IA Public Notice 2. IA Manual Summary 3. IA fiscal Impact |
|

This is my sweet girl, Lila. She’s active and intelligent. She loves to swing, eat blackberries, and paint. Don’t you dare turn your back on her because she’s mischievous too! She loves her friends, family, and kitty-cats. She is absolutely the most wonderful thing I’ve ever done with my life, and she just so happens to have Down Syndrome.

She might smile a lot, but her life hasn’t been easy. Born almost a month early due to multiple complications, Lila spent some time in the NICU. She’s overcome multiple illnesses and surgeries, including open heart surgery soon after her first birthday and many others since. In fact, we have received 2 new diagnoses this year alone, and she’ll have at least one surgery.

My husband and I are proud Arkansans. We’re educated, hard-working, tax-paying citizens. At the time of Lila’s birth, we lived in another state. Despite the fact that we both had good jobs and primary insurance coverage, we struggled to provide for her needs. When we moved back to Arkansas, Lila was significantly delayed in many areas.
 Our friends told us about TEFRA, a type of Medicaid funding that provides for disabled children and that requires the family to pay a premium. Our primary insurance pays first for all that it will cover, and Medicaid makes sure that Lila doesn’t go without the rest. We gladly pay a monthly fee for this essential assistance!
Our friends told us about TEFRA, a type of Medicaid funding that provides for disabled children and that requires the family to pay a premium. Our primary insurance pays first for all that it will cover, and Medicaid makes sure that Lila doesn’t go without the rest. We gladly pay a monthly fee for this essential assistance!
Lila now receives medical treatments that she needs from specialists and Occupational, Physical, and Speech therapy. She attends a school where she is loved and accepted, and they practice important skills in the classroom to prepare her for mainstream Kindergarten. Lila is constantly learning the necessary skills to be independent: speaking new words, learning to feed herself, to dress herself, and to climb stairs. One of my favorite moments was the first time I ever heard her say, “Ma Ma.” Can you imagine waiting 4 years to hear that?
 We never expected to need Medicaid. Even though we’d paid taxes for years for Medicaid, we didn’t know that a person’s life can change drastically in a moment – a car accident, a stroke, a job loss, a cancer diagnosis, a chromosomal difference – to cause them to need Medicaid. We thought that if we worked hard enough, we could take care of ourselves and Lila. But no matter how hard we work or what we give up, we just can’t afford to provide for all of Lila’s needs. Now, because of Medicaid, Lila is thriving, and we’re not being crushed under the weight of Lila’s ever-growing medical debt. We have hope that she will continue to develop and someday be a valued, contributing member of society. We are incredibly thankful for Medicaid.
We never expected to need Medicaid. Even though we’d paid taxes for years for Medicaid, we didn’t know that a person’s life can change drastically in a moment – a car accident, a stroke, a job loss, a cancer diagnosis, a chromosomal difference – to cause them to need Medicaid. We thought that if we worked hard enough, we could take care of ourselves and Lila. But no matter how hard we work or what we give up, we just can’t afford to provide for all of Lila’s needs. Now, because of Medicaid, Lila is thriving, and we’re not being crushed under the weight of Lila’s ever-growing medical debt. We have hope that she will continue to develop and someday be a valued, contributing member of society. We are incredibly thankful for Medicaid.
We tell everyone we can how essential Medicaid is! Lila has visited the Capitol and state lawmakers multiple times to represent herself and friends like her. Since she can’t speak much yet, my husband and I tell them how much Medicaid is literally saving lives. I can’t wait for the day that Lila will tell them herself. She brings a beauty and light to this dark world, and we will never stop fighting for her!



